How Autism Care Actually Scales: A Systems View
Why technology, operations, and markets—not just clinicians—determine access to care
There is a familiar narrative in autism services: access to care scales when we train more clinicians, support them better, and deploy the right clinical tools. This narrative is not wrong—but it is incomplete. And increasingly, it is misleading.
Clinical skill and judgment are foundational. No system compensates for poor care. But when organizations struggle to expand access, sustain quality, or survive payor pressure, the root cause is rarely a lack of clinical commitment or training. The constraint almost always lives elsewhere—in the systems that surround clinicians and shape what they can realistically do.
MissionViewpoint.com exists to examine those systems.
The False Narrative About Scale
When access to care falls short, the instinctive response is to focus on people: recruit more therapists, accelerate training pipelines, reduce burnout, improve supervision. Each of these matters. None of them, on their own, explains why well-intentioned organizations repeatedly hit the same ceilings.
Two quiet assumptions tend to underpin the prevailing narrative:
First, that clinical capacity is the primary bottleneck.
Second, that tools or training can be layered onto existing operations without fundamentally changing how the organization functions.
In practice, organizations often add clinicians into environments that are operationally brittle, administratively overloaded, and technologically fragmented. The result is predictable: utilization leaks, authorization failures, billing delays, supervision strain, and clinician frustration—regardless of how strong the clinical team may be.
Access does not fail because people are unwilling. It fails because systems do not scale linearly with headcount.
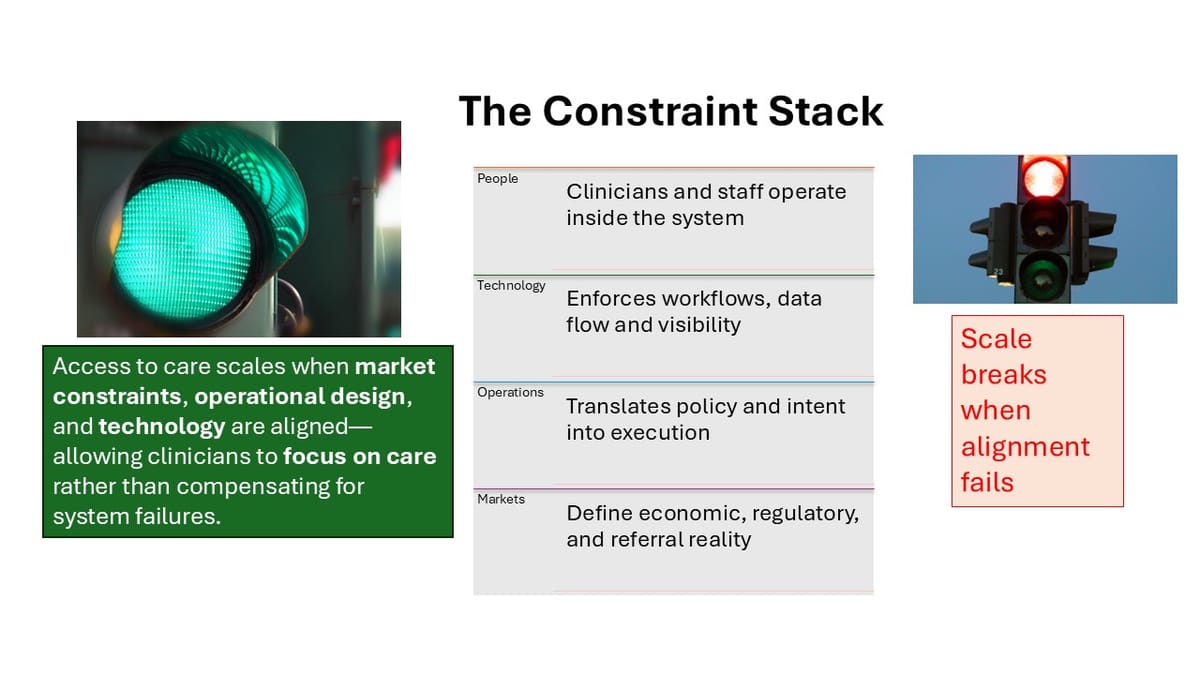
The Actual Constraint Stack
A more useful way to think about scale is as a stack of interdependent constraints. Each layer shapes the one above it, and pressure accumulates where alignment breaks down.
Markets sit at the base. Payors, benefit designs, diagnostic pathways, referral sources, state policy, and network adequacy rules define the economic and regulatory environment. These forces determine which services are viable, how quickly care can start, and where expansion is even possible.
Operations translate market rules into day-to-day reality. Scheduling logic, authorization workflows, supervision models, intake processes, and billing practices determine whether capacity turns into delivered care. Operational design is where theoretical access becomes real—or stalls.
Technology enforces (or undermines) operations. Data flow, workflow design, system interoperability, and reporting determine whether staff spend time delivering care or reconciling systems. Technology does not create strategy, but it powerfully constrains execution.
People operate within everything above. Clinicians, supervisors, and administrators do their work inside the market rules, operational processes, and technological scaffolding they are given. Their effectiveness is shaped as much by system design as by individual capability.
This ordering matters. Many organizations attempt to fix people problems with technology, or operational problems with training, without addressing the underlying constraints. Scale stalls not because effort is insufficient, but because leverage is applied at the wrong layer.
Why This Lens Matters Now
This systems view is not academic. It is increasingly necessary.
Public payors are exerting sustained pressure on rates, documentation standards, and utilization. Commercial payors are tightening authorization logic and shifting financial risk back onto providers. CPT structures continue to evolve in ways that reward certain models of care and strain others. Workforce growth, while real, is uneven and increasingly saturated in some markets while scarce in others.
At the same time, platforms are diverging. Some double down on end-to-end control. Others fragment into point solutions. Many promise efficiency but deliver complexity when layered onto existing stacks. The gap between what tools claim to enable and what organizations can operationalize is widening.
Under these conditions, scale is less about growth ambition and more about structural readiness. Organizations that understand their constraint stack can adapt. Those that do not often mistake symptoms—denials, delays, turnover—for root causes.
How to Read MissionViewpoint
Everything on this site applies this systems lens from different angles.
Briefings surface signals: shifts in policy, platform behavior, operational patterns, and economic pressure. They are not news summaries; they are context for decision-making.
Markets explore the environments in which care is delivered. This includes payor dynamics, diagnostic pathways, referral ecosystems, and regional variation—factors that shape what “scaling” even means in practice.
Providers examine how real organizations navigate these constraints. These are not case studies in success or failure, but windows into tradeoffs, design choices, and operational reality.
Platforms focus on the tooling layer—what systems actually do, what they enforce, and where they break down when exposed to real-world operations.
Read individually, these pieces may seem narrow. Read together, they describe how access to care is created—or constrained—by the interaction of systems.
What This Site Is Not Doing
This work is intentionally bounded.
It is not ranking vendors.
It is not issuing endorsements.
It is not forecasting winners.
It is not marketing dressed up as analysis.
The goal is not to tell organizations what to buy, but to help them understand what they are building—and what they are implicitly optimizing for—before they commit to tools, processes, or growth strategies.
Access to autism care does not scale because of a single breakthrough. It scales when markets, operations, technology, and people are aligned well enough that effort compounds instead of dissipates.
That alignment is difficult. It is rarely visible. And it is where most of the real work lives.
Everything else on this site exists to examine that reality from different vantage points.