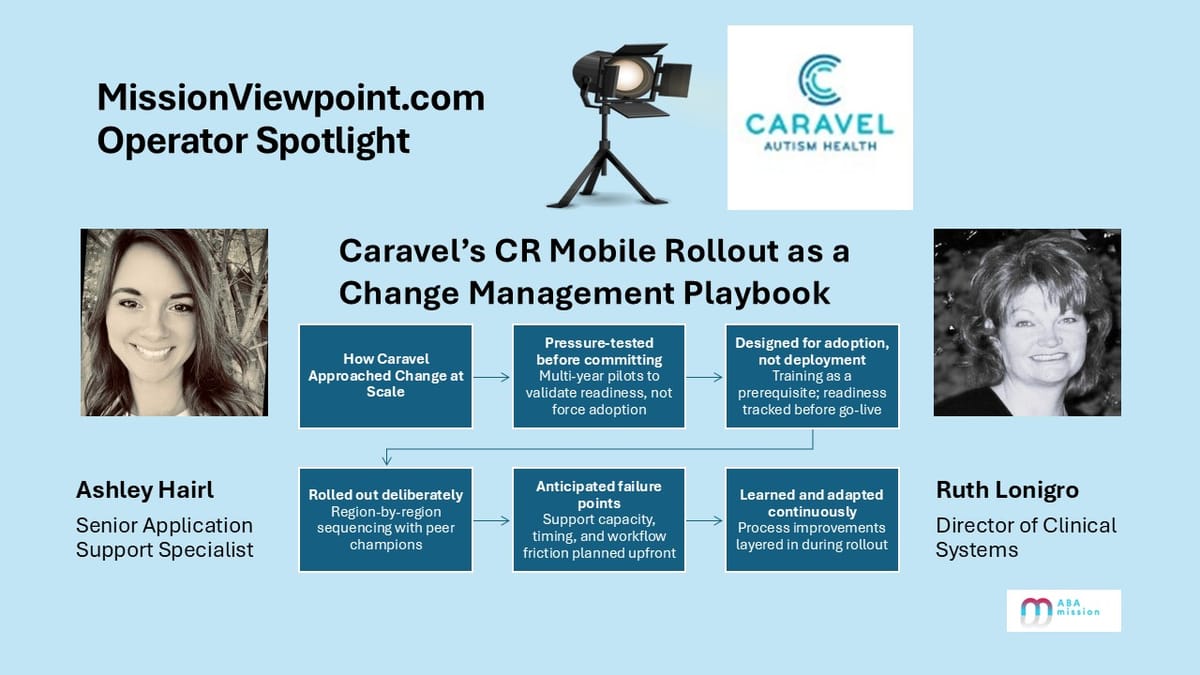
Operator Spotlight: Caravel Autism Health’s CR Mobile Rollout as a Change Management Playbook
Technology stories are straightforward to tell. Change stories are not.
What makes Caravel Autism Health’s CR Mobile rollout worth highlighting isn’t just the adoption of a new capability.
It’s the way the organization approached change itself — deliberately, patiently, and with a clear understanding of the human and operational risks that come with implementing technology at scale.
Large ABA providers face a familiar gauntlet when introducing new systems: executive alignment, frontline skepticism often shaped by prior attempts, training burden, support capacity constraints, and the ever-present risk of disrupting care delivery.
Caravel’s experience stands out because it shows what happens when those challenges are anticipated rather than discovered late, and when learning is built into the rollout rather than treated as a postmortem exercise.
This Spotlight is fundamentally a story about process, discipline, and execution — with technology playing an enabling role, not the starring one.
The people behind the approach
Two leaders were central to how Caravel navigated this change.

Ruth Lonigro, Director of Clinical Systems, brought deep experience in healthcare technology implementation, project management, and instructional design. Her focus on readiness, sequencing, and expectation-setting shaped the structure of the rollout from the start.

Ashley Hairl, Senior Application Support Specialist, anchored execution at the frontline. With a background that spans behavior technician, clinical supervision, and application support, she designed training and support systems grounded in how staff actually work — not how systems are designed on paper.
Together, they treated CR Mobile not as a feature to deploy, but as a program to manage.
The starting point: functional, but not resilient enough
Before rolling out CR Mobile at scale, Caravel’s behavior technicians primarily used the web version of CentralReach on company-issued tablets. The approach worked and supported day-to-day operations, but it carried limitations that became more pronounced as the organization grew.
Connectivity mattered more than it should have. Dead zones within clinics, community-based services, and school settings introduced friction. When data couldn’t be captured cleanly at the point of service, work shifted downstream — often to senior clinicians or administrative teams tasked with reconciliation.
As Ruth explained, the system wasn’t broken — it just wasn’t resilient enough to support the way care was actually delivered across environments.
Caravel wasn’t looking for disruption. It was looking for reliability.
Pressure-testing before committing
Rather than rushing into deployment, Caravel spent a couple of years running pilots and deliberately pushing CR Mobile to reveal where it would hold up — and where constraints still needed to be addressed.
Those early efforts weren’t about proving success. They were about identifying gaps, understanding adoption thresholds, and deciding what conditions had to be met before broader rollout made sense.
“We weren’t interested in forcing adoption,” Ruth noted. “If the experience didn’t meet the bar for frontline staff, no amount of messaging was going to make it stick.”
Over time, continued evolution on the platform side reduced key constraints, and Caravel reached a point where confidence was operational rather than aspirational. At that point, CR Mobile could be treated as a production system — and planned accordingly.
Designing for adoption, not just deployment
Once Caravel committed to rollout, the focus shifted to execution discipline.
Training was treated as a prerequisite, not an afterthought. Ashley built structured education through Relias so staff could understand workflows before using the tool with clients. Completion was monitored weekly to ensure readiness.
“We didn’t want people learning in live sessions,” Ashley explained. “The goal was to remove uncertainty before day one.”
Support was designed to scale. A centralized FAQ became the first line of defense, evolving as new questions surfaced. During go-lives, dedicated Teams channels allowed real-time issue resolution, while post-live check-ins ensured clinics didn’t feel abandoned once the initial wave passed.
Rollout followed a region-by-region approach, with pilot clinics intentionally positioned as peer champions. Timing mattered as well — lessons learned early informed when not to go live, reducing avoidable stress on staff.
The underlying philosophy was simple: anticipate where things might break, and correct course before trust eroded.
When constraints lead to better process
One of the most instructive outcomes of the rollout had little to do with mobile functionality itself.
CR Mobile did not allow session notes to be copied. Rather than forcing workarounds, Caravel used the moment to rethink how note corrections should work altogether.
The result was a session amendment process that improved auditability, reduced burden on behavior technicians, and created a cleaner connection between clinical documentation and timesheets.
“That change ended up helping us beyond mobile,” Ashley noted. “It simplified how corrections happen across workflows.”
Similar second-order benefits emerged elsewhere. Draft timesheets surfaced authorization and coding issues earlier than billing processes typically would, enabling proactive correction even as the team worked through volume management and tooling refinements.
The common thread was a willingness to let implementation expose process gaps — and then address them intentionally.
Learning in motion
Not every lesson was anticipated.
Because clinicians were not primary users of CR Mobile, early training for that group was optional. Over time, it became clear that changes to visibility — particularly around Interobserver Agreement (IOA) workflows and offline behavior — required more explicit communication.
“There were assumptions about real-time access that didn’t translate in an offline-first model,” Ashley said. “Once we understood where expectations didn’t match reality, we adjusted how we trained and supported clinicians.”
Those insights are now incorporated into onboarding and ongoing education, strengthening the organization’s ability to manage future change.
A repeatable model
Caravel’s CR Mobile rollout wasn’t successful just because a product improved — though that mattered. It worked because the organization treated change management as a core capability: one that improves through iteration, reflection, and disciplined execution.
As Ruth put it, “Every rollout teaches us something. The goal is to carry those lessons forward.”
In a market where technology adoption is inevitable and trust is hard-earned, that mindset may be one of the most scalable advantages of all.