Operator Spotlight: SpringHealth Behavioral Health: Bridging Gaps Across Age and Care Models
Building a continuum of care for a population most providers stop serving at 21
Tabitha Chapuran started SpringHealth in February 2017 with eleven staff and a handful of adults on home and community based waivers. She wasn’t trying to build an ABA company. She was trying to fill a gap she had been watching widen for more than two decades.
The gap was not hard to find. Most autism providers are built around a straightforward assumption: intervene early, focus intensely, and discharge once meaningful progress is made.
The clinical logic is sound, and the financial incentives reinforce it. Reimbursement is most reliable for young children. Outcomes are most measurable in that window. The system tends to reward concentration, not continuity.
What happens after that is less clear — and far less supported.
For individuals who age out of pediatric services, the structure that once surrounded them tends to fragment. ABA becomes harder to access in most states. Mental health services operate separately, if at all.
Residential providers carry the day-to-day burden without specialized behavioral support. The need doesn’t disappear. It changes shape, and in many cases becomes harder to address.
Tabitha had seen this up close. Before founding SpringHealth, she spent nearly a decade working at a large intermediate care facility for adults with intellectual and developmental disabilities, at a time when such facilities housed close to 400 people.
She later served as the psychological program administrator for the state of Kentucky, providing oversight across state-funded mental health and IDD programs and engaging directly with Medicaid on waiver implementation.
That experience didn’t produce a market thesis. It produced a sense of obligation.
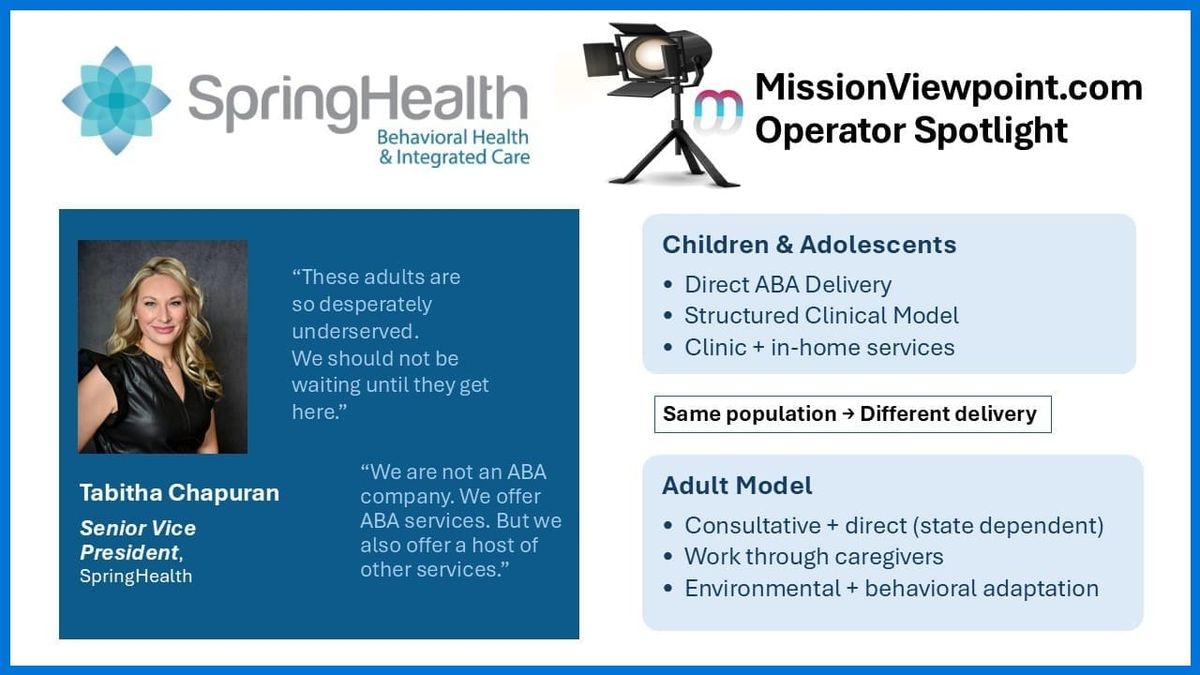
“These adults are so desperately underserved. We should not be waiting until they get here. Let’s get in there earlier.”
What started as a consultative service supporting adults in residential settings gradually extended backward — into youth services, clinic-based care, and eventually a model that now spans twelve states, roughly 750 employees, and a population served from age 2 to, as Tabitha puts it (to my surprise), about 87.
Not an ABA Provider
The distinction matters to Tabitha enough that she makes it explicitly — including at job fairs, where prospective hires often assume the label.
“We are not an ABA company. We offer ABA services. But we also offer a host of other services. And I think we are one of very few companies actually trying to create this.”
SpringHealth is organized around a population, not a modality.
ABA is a tool — an important one — but not the organizing identity of the organization. The identity is the population: individuals with developmental and intellectual disabilities, across the full arc of their lives.
When SpringHealth began expanding into youth services and needed an electronic health record capable of supporting multiple disciplines, Tabitha evaluated a platform built specifically for ABA — and walked away.
“It looked like it was going to be a great program for an ABA company,” she said. “But we’re not an ABA company.”
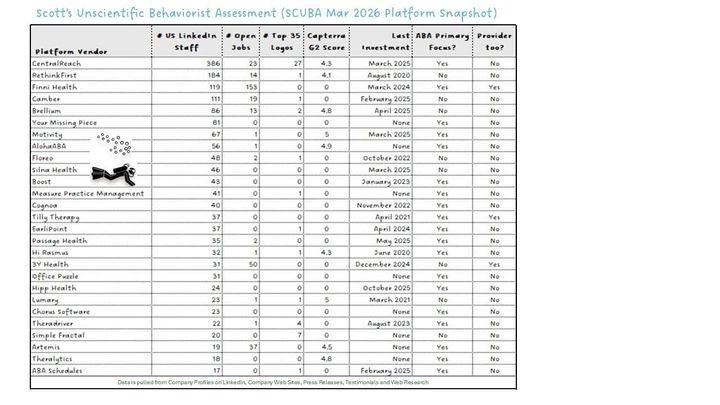
The search eventually landed on Rethink Behavioral Health, chosen specifically for its flexibility to support documentation across disciplines — ABA, speech therapy, occupational therapy, mental health — without forcing each into an ABA-shaped workflow.
The speech language pathologist could write a note that reflected her discipline. The mental health clinician could document without feeling boxed into a behavioral framework. All of it lived in the same system.
“I needed an EHR where I could integrate all therapy types under one umbrella. I would not go with two or three different systems. That was not going to happen.”
Five years later, that system holds the organization together — scheduling, documentation, data collection, billing, HR — across twelve states and two very different operating models.
Two Operating Systems
SpringHealth’s youth and adult service lines run on different clinical and operational logic, shaped less by preference than by constraint.
For children and adolescents, the structure is recognizable:
- in-home and clinic-based ABA
- behavior technicians under supervision
- standard authorization and billing workflows
For adults, the model becomes conditional.
In states that permit direct behavioral services for adults — Missouri is one example Tabitha cites — the model resembles a scaled version of pediatric ABA. Clinicians work directly with individuals, often those in their thirties or forties who never received services when younger.
In states where funding restricts the adult model to consultative services, the approach shifts. SpringHealth clinicians — BCBAs and psychologists — go into residential settings and work through the people who are with the individual every day: direct support professionals.
They train those staff, help them understand behavior, and design interventions that can be implemented consistently without being physically present.
“We don’t have behavior technicians for the adult line because most states don’t allow for it. So, we’re using the resources that already exist — and training them.”
“The environment changes everything… you have to adapt to what’s actually happening around the individual."
Even within the same discipline, application changes.
Occupational therapy for a five-year-old is hands-on intervention. For an adult, it may be environmental adaptation — modifying a home, introducing adaptive equipment, or redesigning routines to enable independence.
The discipline is the same. The work looks very different.
What appears to be a single organization is, in practice, operating across two systems — each shaped by reimbursement, workforce, and setting.
The model also serves a secondary purpose: expanding clinician exposure to adult populations, where many providers have historically had little experience.
Growth Without a Marketing Budget
SpringHealth’s expansion has been almost entirely organic.
“We know the need is there. We’ve often started in very rural areas and just grown from that.”
There is no dedicated marketing function. No heavy acquisition strategy. No M&A-driven scale.
The one exception was a recent acquisition in North Carolina — an ABA company that became a tuck-in.
The outcome reflects the model more than a traditional acquisition strategy. The organization continued its ABA operations and now also serves over thirty adults — many of whom would not have otherwise had access to behavioral services.
Clinicians who had only ever worked with children began working with adults, extending the model not just operationally, but culturally across the workforce.
“We see it as part of our mission to try to educate and expand the workforce. These kids are going to become adults. They need people who know how to help them as they get older.”
The model didn’t replace what existed — it extended it.
Referrals for youth follow expected channels — insurance, families, providers.
For adults, the path is different.
Residential providers call when they’ve reached the limits of what they can manage internally. SpringHealth fills that gap.
The result is a model that scales not through consolidation, but through demand.
Operating Ahead of the System
The tension running through this model is structural.
The clinical logic for a continuum is obvious. The operational reality is not.
Reimbursement for adult behavioral services remains inconsistent. In most states, ABA for adults simply isn’t billable. Consultative models are permitted but underfunded — sometimes limited to one or two hours per month.
The system was not designed for continuity. It was designed for early intervention.
SpringHealth operates within those constraints rather than waiting for them to change.
“The adult services are not well resourced. But you can’t just abandon this population when they become 21.”
That choice defines the model.
Not because it is efficient — but because it is necessary.
What This Signals
SpringHealth’s model is not yet the dominant structure in autism care. But it points toward a gap the market has not resolved.
As more individuals who received early intervention age into adulthood, the expectation of continued support will follow.
The current structure is unlikely to hold.
Over time, adult care will move toward the same kind of convergence pediatric autism care already experienced — more defined models, more consistent funding, and tighter coordination across services.
When that happens, early intervention will no longer be a phase of care.
It will be the beginning of one.