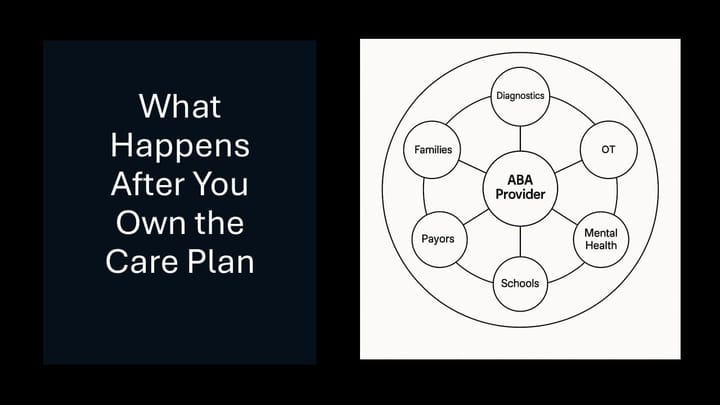
The Hidden Cost of Building Your Own Stack in the Age of AI
AI has changed the economics of software creation. Tools that once required large engineering teams can now be prototyped quickly. Workflows can be automated. Interfaces can be stitched together. For autism providers, this creates a tempting conclusion:
If software is easier to build, maybe we should build more of it ourselves.
That instinct is understandable—and sometimes correct. But it comes with a set of second-order risks that are often underestimated, especially in healthcare delivery organizations.
The AI Acceleration Fallacy
The current wave of AI tooling lowers the cost of writing code, not the cost of operating software.
Providers evaluating build-versus-buy decisions often focus on:
- Speed of development
- Flexibility of customization
- Avoiding vendor lock-in
What receives less attention is the cognitive and organizational load introduced once a provider becomes the system integrator, product owner, QA team, and long-term maintainer of their own stack.
In autism services, that load compounds quickly.
Orchestration Is the Scarce Resource
AI-enabled tools are increasingly accessible. The scarce capability is orchestration:
- Translating clinical and operational needs into coherent requirements
- Iterating with real users to refine those requirements
- Managing dependencies between data, workflows, and edge cases
- Testing in environments where errors have compliance and revenue impact
People who are good at this work—true systems thinkers who can bridge operations, data, and technology—are difficult to hire in any market. In autism care, the challenge is sharper:
- These roles are paid more competitively in traditional tech companies
- The work inside provider organizations is messier, slower, and constrained by payors and regulation
- The upside is often limited unless the provider is already operating at significant scale
As a result, many providers attempting to “build their own stack” are functionally under-resourced in the very role that matters most.
Requirements Are Not Static in Healthcare
Even when providers do secure technical talent, another challenge emerges: requirements instability.
AI systems are only as good as the assumptions embedded in them. In autism services:
- Workflows differ by state, payor, and care model
- Policies change mid-year
- Clinical judgment does not always map cleanly to deterministic logic
Distilling durable requirements requires repeated iteration with business users who are already stretched thin. Each iteration consumes attention that would otherwise go toward:
- Clinical supervision
- Hiring and onboarding
- Payor negotiations
- Family communication
Over time, the technology becomes the work—not the enabler of it.
Testing, Maintenance, and Model Drift
AI-driven systems introduce ongoing operational risk:
- Models drift as data distributions change
- Automations break when upstream systems change
- “Small” fixes cascade into unexpected downstream effects
This is manageable—but only with disciplined testing, monitoring, and maintenance practices. In most provider organizations, those practices are immature or nonexistent, not due to negligence, but due to focus.
Autism providers are care organizations first. They are not software companies.
Data Sophistication Is a Prerequisite, Not a Given
There is also an unspoken dependency in many AI narratives: data readiness.
To support AI agents that do more than automate tasks—agents that inform what to do next—providers need:
- Consistent, well-modeled operational and clinical data
- Clear data ownership and access patterns
- Governance around how data is used, corrected, and interpreted
Very few providers, even large ones, are starting from this position.
Two Legitimate Uses of AI for Providers
It helps to separate AI use cases into two categories:
- AI for Operations
- Documentation support
- Revenue cycle automation
- Scheduling, eligibility, and authorization workflows
- AI for Intelligence
- Identifying risk
- Prioritizing action
- Informing strategic and clinical decisions
Most providers can and should benefit from the first category today. The second requires significantly more infrastructure, maturity, and sustained investment.
Why Vendors Should Carry the Table Stakes
For the majority of providers, the pragmatic path is not to avoid AI—but to delegate its complexity.
That means:
- Selecting tech platforms that are deeply grounded in ABA workflows
- Ensuring access to underlying data, not just surface-level dashboards
- Evaluating vendor roadmaps with the same rigor applied to clinical expansion
Vendors should deliver AI-enabled table stakes reliably and safely. Where those capabilities also support differentiation, that is additive—but not required.
True differentiation is often better pursued selectively, where providers have unique insight and sufficient scale to justify the investment.
A Familiar Pattern Among Tech-Savvy Providers
This tradeoff is already visible in the market.
Even smaller, operationally sophisticated providers have experimented with highly customizable tools—workflow platforms, low-code systems, and flexible task engines. Many initially succeeded in bending these tools to their needs.
Over time, however, a pattern emerged:
- The cognitive load of maintaining the system increased
- Key staff became de facto product managers
- Attention drifted away from care delivery, workforce stability, and payor relationships
Several ultimately chose to step back—not because the tools failed, but because the cost of ownership did.
The Decision Is Not About Capability—It’s About Focus
None of this argues against ambition or technical literacy. It argues for clarity of focus.
Building and operating software is a business. Delivering autism care at scale is another. A small number of providers may successfully do both. Most should not try .... at least not yet.
The hardest technology decision providers face today is not whether AI is powerful enough.
It is deciding where its complexity belongs.
Decision Summary
Autism providers should consider building AI-enabled systems internally only if they meet most of the following conditions:
- Operate at significant scale (multi-state or enterprise)
- Have dedicated product, data, and integration leadership—not shared roles
- Control well-structured, high-quality operational and clinical data
- Can sustain ongoing testing, monitoring, and iteration as models and workflows change
- Are willing to absorb the cognitive and organizational cost of long-term ownership
For most providers, AI value is better realized by delegating complexity:
- Select platforms with deep fluency in ABA workflows and regulatory realities
- Prioritize data access, governance, and interoperability over surface-level features
- Expect vendors to deliver AI-driven table-stakes capabilities reliably
- Reserve internal technology investment for narrow, defensible differentiators—where scale and insight justify the effort