📬ABA Mission Viewpoint Monthly Update – January 2026

The Mission of ABA Mission
👉To drive more—and better—access to ABA care through the smarter use of technology and data.
Welcome to the ABA Mission Viewpoint January 2026 Monthly Update
Theme: Operational Resilience
December focused on Infrastructure Readiness — the systems that shape access, coordination, and cost in autism care.
January shows whether that readiness was real — and this January is testing it more than most.
Payor margin pressure is higher and more immediate than at any point in recent memory, accelerating changes to benefit design, authorization logic, documentation expectations, and enforcement posture. Layered on top of the usual January resets — expiring authorizations, shifting family financial behavior, tighter workforce utilization — the result is a concentrated stress test across the ABA operating stack.
What emerges is less about what changed and more about what holds. Systems that functioned under steadier conditions are being pushed to respond faster, with less tolerance for ambiguity and rework. Execution discipline matters more than plans. Infrastructure determines whether disruption is contained or cascades.
Across payors, platforms, providers, and investors, a consistent signal is forming. The next phase of ABA delivery will not be defined by scale or tooling alone, but by whether systems absorb pressure without passing instability downstream — to clinicians, families, or access to care.
That question — what holds, and what breaks — is the throughline of this issue.
🧩 How Autism Care Actually Scales
Under pressure, familiar explanations resurface. When access tightens or growth slows, the conversation often defaults to clinician supply: not enough therapists, supervisors, or training capacity.
That framing is understandable—but increasingly insufficient.
January makes visible that access rarely breaks first at the clinical layer. It breaks earlier in the systems that determine whether capacity can be scheduled, authorized, supported, and sustained. Staffing plans collide with authorization constraints. Utilization assumptions unravel under payor resets. More people do not automatically translate into more delivered care.
This brief reframes scale as a systems problem rather than a headcount problem. It examines how markets, operations, and technology either convert effort into access—or dissipate it through friction. When those layers are misaligned, growth amplifies instability. When they are designed intentionally, capacity compounds.
January’s pressure sharpens the distinction. Organizations with similar clinical talent are experiencing very different outcomes based on how well their systems absorb variability.
Takeaway:
Access to autism care scales when systems—not just people—are built to translate capacity into delivery under real-world constraints.
📅 January Payor Readiness: When Assumptions Expire
Every January introduces change. This one is amplifying it.
Coverage structures reset. Authorizations expire or shift. Deductibles reappear in family decision-making. Under current margin pressure, payors are less tolerant of ambiguity and slower remediation. What once surfaced as downstream cleanup now shows up immediately as utilization loss or delayed cash flow.
The core issue is rarely eligibility itself. It is the assumption that coverage and authorizations are static, rather than living states that require ownership and enforcement.
January functions as a recurring operational stress test. It reveals whether organizations manage eligibility and authorization proactively—or allow assumptions to decay until claims fail. Platforms can assist at points in this chain, but they do not replace a defined operating model.
This analysis focuses on what consistently works: treating January as a managed operating season, leading with process discipline, and using technology as an accelerator rather than a substitute.
Takeaway:
January disruption is not an intake nuisance. It is a measure of operational maturity under pressure.
🏰 Investor Moats: Why Structural Defenses Break First
Volatility exposes false certainty. In ABA, that often shows up in how “moats” are defined.
Clinic density, reimbursement rates, and geographic position are still commonly cited as defensive advantages. In stable conditions, they can appear durable. Under sustained pressure, they are often the first to erode.
Payor behavior is shifting quickly across state Medicaid programs. Authorization logic is tightening. Reimbursements are declining through increased friction rather than just headline cuts. Organizations relying on structural advantages alone are feeling the strain immediately.
What holds instead are capabilities: detecting change early, adapting workflows quickly, protecting clinician time, and maintaining financial visibility. These traits are less visible than footprint, but they compound under pressure.
Takeaway:
In ABA, the most durable moats are operational capabilities—not structural positions that assume stability.
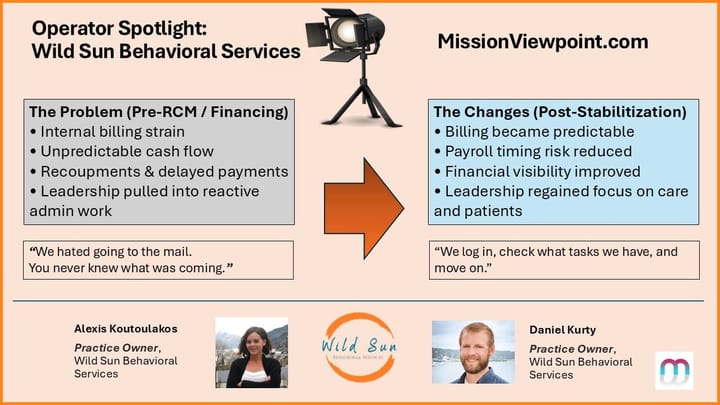
💡 Operator Spotlight: Jaybird ABA
Periods of pressure tend to pull leadership away from the floor. Administrative load increases, decision-making drifts upward, and clinical leaders spend more time managing systems than supporting care teams.
Jaybird ABA is instructive because it was designed to resist that drift.
Rather than scaling first and retrofitting later, Nicola Brummer of Jaybird aligned an operating model around a clear priority: protecting clinical leadership proximity while absorbing operational friction early. Administrative burden is handled by Finni upstream, workflows are designed before growth, and leadership time is deliberately preserved for supervision, mentoring, and culture.
This matters most in moments like January. When payor dynamics tighten and operational assumptions break, organizations that rely on heroics tend to push stress downstream. Jaybird’s model contains disruption instead—allowing clinicians to stay focused on staff and families rather than reacting to system noise.
Takeaway:
Operational design that protects clinical leadership time is not a luxury. It is a stabilizing force under pressure.
✅ Platform Highlights
- Accreditation consolidation — CASP acquired Jade Health (including BHCOE), consolidating organizational accreditation under ACQ. CASP has acknowledged overlapping benchmarking initiatives, noting that the future structure and branding of NADR-like efforts remain under consideration.
- Theralytics completed a SOC 2 Type II audit.
- Artemis launched Insurance Discovery to identify undisclosed or inactive coverage across commercial, Medicaid, and Medicare plans.
- Flychain and TheraDriver announced a strategic partnership.
- Passage Health introduced goal grouping and expanded multi-data programming capabilities.
- CircaThera rebranded from ABA Toolbox.
📊 Provider Trends
Culture as a Differentiator Within Scale
- Across the Top 20 ABA providers, LinkedIn headcount increased ~21% over 2025; at the cohort level, growth and Glassdoor ratings showed no simple linear relationship.
- Among the Top 5 providers, all posted above-average Glassdoor ratings and above-average growth relative to the Top-20 baseline.
- A fast-growing mid-tier cohort — including SOAR Autism Center, Yellow Bus ABA, Achievements ABA, Positive Development, Golden Steps ABA, Brighter Strides ABA, Behavioral Framework, and Akoya Behavioral Health — showed materially higher Glassdoor ratings (low-to-mid 4s) alongside sustained growth, averaging ~0.7–0.8 points above the Top-20 baseline.
Takeaway:
As organizations scale, culture and execution discipline increasingly separate growth outcomes — particularly at the very top and just below the largest tier.
💬 Closing Thoughts
January has a way of clarifying things. This January - even more so.
When assumptions reset all at once—around payors, authorizations, staffing, and cash flow—what matters most becomes visible quickly. Not strategy decks or tool inventories, but whether systems absorb pressure or pass it downstream. Whether leadership time stays anchored to care delivery or is consumed by rework. Whether execution holds when conditions tighten.
This month’s work points to a consistent conclusion: resilience in ABA is not accidental. It is designed. It shows up in how organizations structure ownership, enforce workflows, protect clinical focus, and respond to change before it cascades.
Despite intensified margin pressure, the field is not retreating. Demand remains strong. Innovation continues. What is changing is the tolerance for fragility. Providers, platforms, and investors are increasingly sorting not by scale alone, but by execution quality under stress.
Until next time,
— Scott
P.S. Know someone shaping ABA operations, technology, or investment? Invite them to subscribe at missionviewpoint.com.
Not sure it's worth your time? Check out our reader testimonials.
Subscribe here.