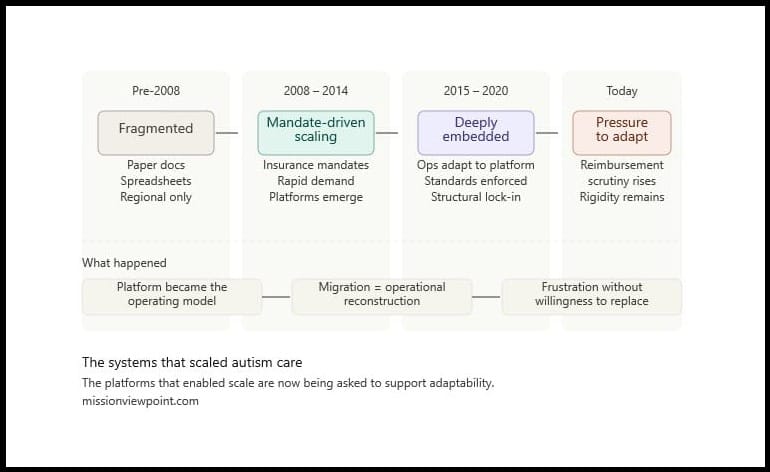
The Systems That Scaled Autism Care
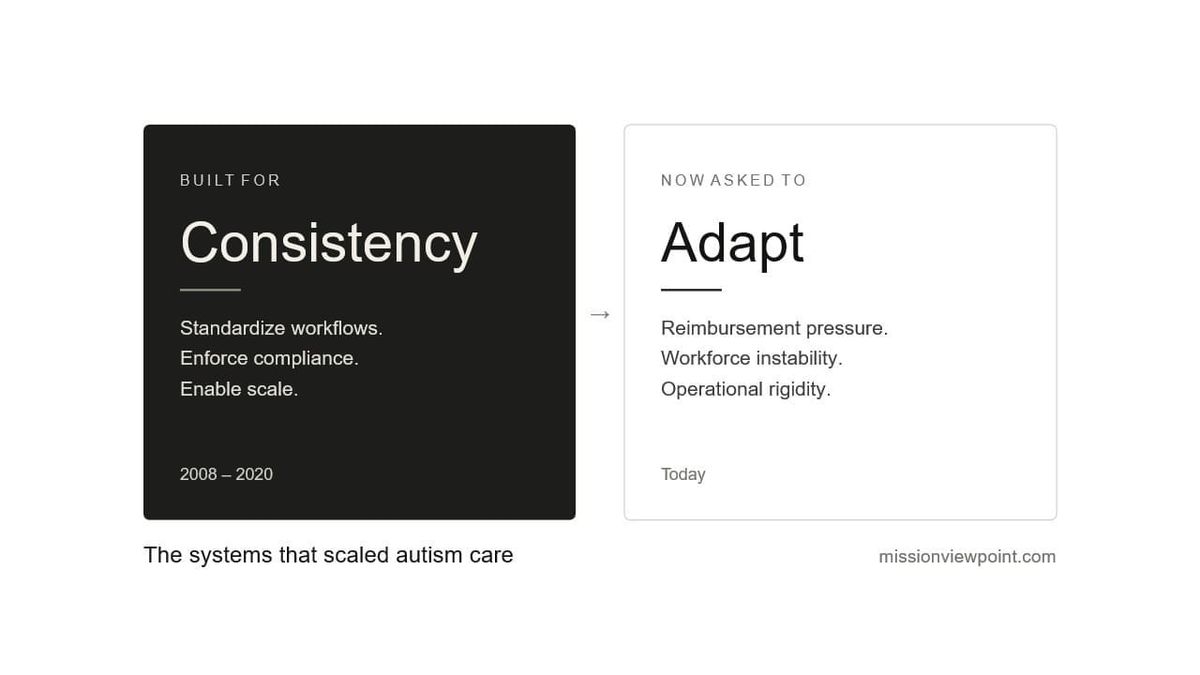
The platforms that enabled scale are now being asked to support adaptability.
Before autism care became a scaled healthcare industry, it was operationally fragmented.
There were no broadly adopted enterprise systems supporting autism care operations. No standardized operational workflows across the industry. No meaningful interoperability expectations. In many organizations, there was not even a consistent operating model.
Clinical documentation was often captured on paper. Scheduling frequently lived in spreadsheets, whiteboards, or localized systems. Billing processes were heavily manual. Supervision structures varied significantly between providers. Administrative coordination depended more on institutional knowledge than operational infrastructure.
And at the time, that environment was largely sufficient.
The industry itself was still relatively small. Most providers operated regionally. The pressure to standardize workflows across multiple states, locations, and payor environments had not yet fully emerged.
Then the market changed.
When autism services scaled rapidly, platforms scaled with them.
And over time, they became embedded in ways that are now very difficult to undo.
That embedding did not happen because providers made poor decisions.
It happened because the systems solved real operational problems during a period when the industry urgently needed operational consistency.
Beginning in the late 2000s and accelerating through the early 2010s, insurance mandates dramatically expanded access to autism services across the United States. Demand increased rapidly. Organizations that previously operated at relatively modest scale suddenly faced pressure to coordinate scheduling, billing, supervision, authorizations, and documentation across increasingly complex operations.
The industry needed infrastructure quickly.
Not theoretical infrastructure.
Operational infrastructure.
A small number of platforms stepped into that vacuum.
Most initially emerged from the clinical side of the business. Data collection, session documentation, treatment execution, and supervision tracking represented some of the earliest areas of operational digitization. Over time, several of those systems evolved into increasingly comprehensive operational platforms spanning scheduling, billing, authorizations, payroll coordination, supervision tracking, and reporting.
The progression was logical.
Clinical systems needed stronger administrative integration. Administrative systems needed better clinical visibility. Providers wanted fewer disconnected workflows. Centralization became increasingly valuable as organizations scaled.
At the time, nearly any improvement over the existing operational state created meaningful value.
A platform that reduced paper documentation mattered. A system that centralized scheduling mattered. Digitized supervision tracking mattered. Scalable claims workflows mattered.
The market was not evaluating these systems primarily through the lens of long-term architectural flexibility or interoperability.
It was evaluating whether organizations could function at scale.
And increasingly, they could.
As the industry matured, broader operational standards began to emerge around the platforms themselves.
Payors developed more formal authorization expectations. States introduced increasing documentation and compliance requirements. The BCBA credential expanded significantly as the field professionalized. The RBT role introduced more standardized frontline workforce expectations across providers.
Organizations such as Council of Autism Service Providers and Behavioral Health Center of Excellence helped push the industry toward greater operational consistency around supervision, training, documentation, and care delivery expectations.
These developments did not occur separately from the platform layer.
The platforms increasingly became one of the mechanisms through which those standards operationalized at scale.
Supervision tracking became more measurable because systems could structure and enforce it. Documentation became more standardized because platforms normalized required workflows. Scheduling structures became more repeatable because operational rules became embedded into software logic.
In many organizations, the platform became part of how the operating model itself was enforced.
Capabilities expanded accordingly.
Platforms evolved from relatively focused clinical or scheduling tools into increasingly comprehensive operational systems supporting authorization management, documentation standardization, supervision requirements, scheduling coordination, payroll integration, reporting, credential tracking, and compliance workflows.
Most of these systems were not originally designed around modern interoperability or data architecture assumptions.
They were built from a function-first perspective.
The goal was workflow execution.
Can sessions be scheduled? Can notes be completed? Can claims be submitted? Can supervision be tracked? Can operational consistency be enforced across locations?
Those were the problems the market needed solved.
And for many years, the architecture underneath mattered far less than the operational outcomes on top.
Interfaces were limited. Data models evolved incrementally. Interoperability was secondary. Reporting was often constrained by the assumptions embedded inside the platform itself.
None of this was unusual for the period.
Inside autism care specifically, that consistency was badly needed.
The platforms did not merely support operations.
Over time, operations adapted to them.
Organizations trained staff around platform logic. Clinical supervision structures aligned to available workflows. Scheduling teams developed operational habits around system constraints. Reporting structures formed around available fields and outputs. Administrative escalation paths evolved around platform limitations and workarounds.
Eventually, the distinction between the organization's operational model and the platform itself became increasingly difficult to separate.
The software stopped behaving like an application supporting operations.
It became part of the operating model itself.
This became especially true as providers scaled through the mid-2010s and beyond.
Larger organizations accumulated years of payor-specific logic, scheduling exceptions, staffing rules, supervisory adaptations, and reporting workarounds around their systems.
Many providers were no longer operating standardized versions of workflows.
They were operating deeply customized operational ecosystems shaped partially by the realities of their business and partially by the assumptions embedded inside the platform.
That dependency became structural.
Not because providers irrationally resisted change.
Because continuity mattered.
A scheduling disruption affects care delivery. A claims disruption affects payroll. A documentation disruption affects compliance exposure. A reporting disruption affects operational visibility.
The larger the provider, the greater the accumulated operational surface area attached to the platform layer itself.
Which is why many providers simultaneously experience frustration with incumbent systems while remaining highly reluctant to replace them.
Outside observers often interpret this as market inertia.
Usually it is risk management.
Replacing a deeply embedded platform is not simply a software migration.
It is an operational reconstruction project touching scheduling, billing, payroll, clinical documentation, authorizations, reporting, supervision structures, staff training, and historical operational logic simultaneously.
Even when a newer platform is objectively cleaner, more modern, or more flexible, the migration risk can outweigh the perceived operational upside.
The architecture worked well enough for the environment in which it emerged.
It created order. It enabled scale. It standardized workflows. It helped transform autism care from a fragmented regional service model into a more operationally coordinated healthcare industry.
That was the right outcome for that moment in the industry's evolution.
The question now is what happens when the environment changes — and the infrastructure can't easily change with it.
That's where the industry is today.
This is the first in a three-part series around this month's theme of "Your job demands innovation. Your operations and tech stack resist it."
Next: how technology often reshaped provider operations — and why many organizations now struggle to adapt around it.