Why Autism Care Coordination Breaks — Systems That Don’t Function as One
This is the first piece in a series examining how autism care is delivered across systems—and why it isn’t designed as one.
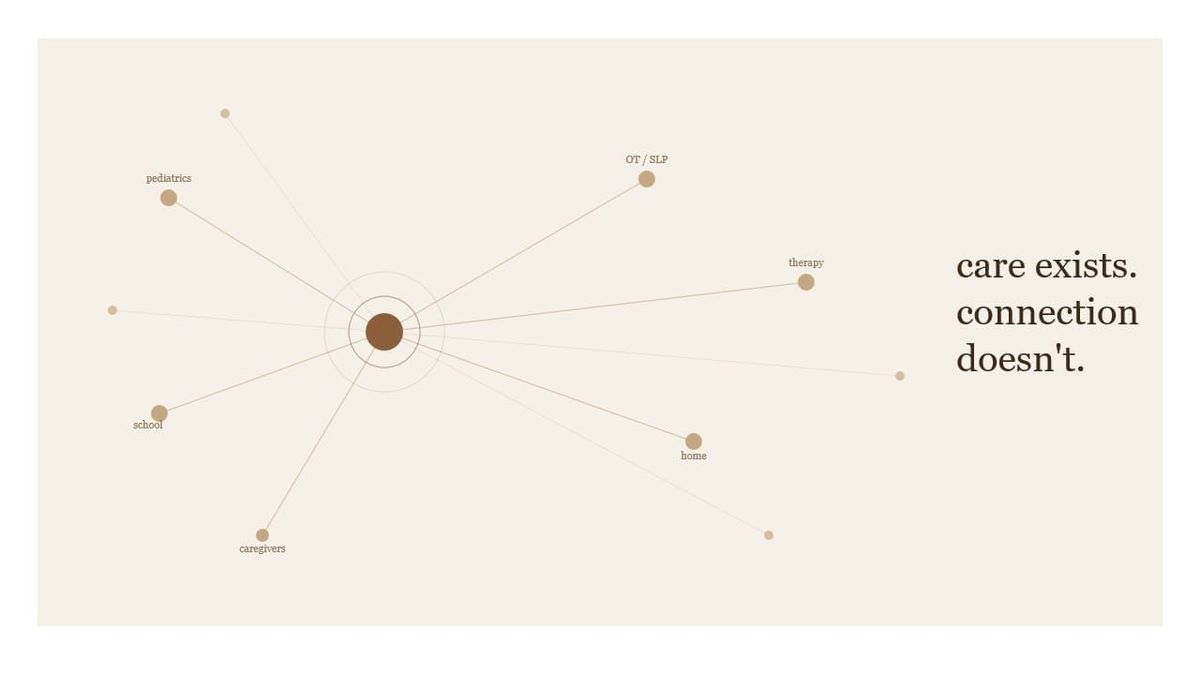
Autism care is delivered across multiple settings, each operating on different systems.
ABA, therapy services, schools, and medical care often serve the same individual on the same day.
Those systems are not designed to function as one.
Coordination is required.
No system provides it.
The System Requires Coordination. It Doesn't Provide It.
Autism services span multiple domains simultaneously:
- Pediatricians → diagnosis and overall health
- RBT's, BCBAs → behavioral intervention
- SLP, OT, PT → developmental goals
- Schools → educational responsibility via IEPs
- Caregivers → daily implementation across all of it
Each operates:
- on different timelines
- under different reimbursement models
- with different definitions of what progress looks like
This is not a single system of care.
It is a set of parallel systems operating on the same patient — with no mechanism designed to hold them together.
Coordination is required.
No system owns it.
The Gap Opens at Diagnosis — and Rarely Closes
The coordination failure begins earlier than most operators recognize.
It starts at diagnosis.
Pediatricians diagnose or refer for diagnosis, initiate care pathways, and remain medically responsible for the child's overall health.
In a coordinated system, they would have visibility into:
- what services are being delivered
- how the child is progressing
- how care plans are evolving across disciplines
In practice, that visibility rarely exists.
After diagnosis, care moves into ABA platforms, therapy-specific systems, and school-based environments.
The physician responsible for the child's health has no structured window into the largest category of intervention being delivered — no consistent view of:
- intervention intensity
- skill acquisition
- plan changes
- cross-setting performance
The system that diagnoses autism is not the system that delivers it.
And there is no mechanism that reconnects them.
That gap doesn't close as the individual gets older — it widens.
The transition to adult services is one of the most fragmented moments in the autism care continuum. School-based supports end. ABA coverage becomes harder to sustain. Adult services operate under entirely different funding structures, eligibility requirements, and provider networks.
Whatever coordination existed in childhood — however imperfect — largely doesn't transfer. Families describe it as starting over. Clinically, that's often exactly what it is.
The coordination failure isn't a childhood problem.
It's a lifespan problem with no systemic solution at either end.
This Is a Design Problem, Not an Integration Problem
The lack of coordination is often framed as a technology integration breakdown.
It isn't.
It's a system design problem.
ABA platforms are built around:
- sessions and supervision structures
- authorization-linked billing
- continuous intervention with discrete measurable units
Medical EHRs are built around:
- encounters and diagnoses
- orders and medications
- episodic events with defined inputs and outputs
School systems are built around IEP objectives and educational timelines.
These are not different implementations of the same system.
They are genuinely different systems.
They are built on different models of what care is, how it progresses, and what counts as a result.
There is no shared unit of care across these systems.
No common structure for how progress is defined, measured, or updated over time.
Even when integrations exist, they move data without aligning meaning. An ABA session note does not map cleanly to an encounter or a clinical order.
The systems can exchange information.
They cannot operate on the same model of care.
The Financial Model Reinforces the Problem
The reimbursement system pays for units of service.
It does not pay for coordination across them.
Each participant optimizes locally:
- deliver authorized hours
- document for compliance
- maintain margin
No one is accountable for:
- total outcome
- continuity across settings
- longitudinal trajectory
Coordination becomes unpaid work. It gets absorbed inconsistently by staff — or pushed onto families.
This is why the problem persists even when individual providers are doing their jobs well.
The incentive structure funds the silos.
It doesn't reward the connective tissue.
No One Owns the Whole Patient
Each system owns a portion of care:
- ABA providers own behavioral intervention
- therapists own discipline-specific goals
- schools own educational progress
- physicians own medical oversight
But no system owns:
- the full care plan
- coordination across settings
- longitudinal progress
Care is delivered across systems.
Ownership is fragmented across them in exactly the same way.
There Is No Shared Definition of Success
Each part of the system measures something different:
- ABA → skill acquisition
- SLP → communication gains
- Schools → IEP progress
- Payors → utilization and cost
- Families → independence and stability
These measures are not wrong.
They are simply not reconciled with each other.
Without a shared definition of success:
- outcomes cannot be aggregated
- performance cannot be benchmarked
- value-based care has no foundation to stand on
This is why value-based care is a perennial conference topic in autism — and why it rarely moves beyond the panel discussion.
The concept is sound.
The structural conditions to support it don't exist.
You cannot contract for outcomes you have no consistent way to measure, across systems that don't share a model of what progress looks like.
The organizations that have gotten closest — Cortica is the clearest example — have done so through significant custom infrastructure investment.
They built the coordination layer themselves: integrated care teams, shared clinical records, aligned incentives across disciplines under one model.
It works.
But it required building something the broader system doesn't provide — and it isn't easily replicated without the same level of organizational commitment and capital.
That's the real signal.
When the best illustration of what coordinated autism care could look like required a ground-up rebuild to achieve it, the gap isn't incremental.
It's structural.
A Coordination Layer Is Missing — and Starting to Take Shape
What’s absent is a layer responsible for maintaining a shared, accessible view of care across these environments.
Not a system that replaces what exists.
Not a direct integration between platforms built on incompatible models.
Something different — a shared surface where care summaries, progress signals, and communication across disciplines can live in a form that everyone involved can actually use.
Emerging approaches—often using AI—are beginning to translate across these systems, turning session-level data into summaries that can be understood outside the platform they were created in.
That is the gap.
Autism care is not failing within systems.
It is failing between them.
Autism care is delivered across systems that were never designed to function as one.
No system owns coordination. No model supports it.
The next question is what happens when one system — like ABA — tries to fill it alone.
And after that, what a real coordination layer would need to look like to work.
MissionViewpoint covers the intersection of technology, operations, and markets in autism care. Subscribe at missionviewpoint.com.