
The Road From Medicaid Pressure Leads Directly to Prior Authorizations
The reimbursement pressure across autism care is obvious.
Providers feel it.
Platforms are repositioning around efficiency and automation.
Investors are increasingly evaluating sustainability and durability.
None of that is difficult to see.
What may be less obvious is how those pressures are likely to reshape the behavior of the ecosystem itself.
Over the past few weeks, I attended both CASP and AIS West 2026. Across dozens of conversations with providers, operators, platform leaders, and investors, I found myself thinking less about the immediate reimbursement debate—and more about the second-order effects.
Because the autism services ecosystem did not originally evolve around mature efficacy measurement systems. It evolved around access expansion.
For years, that largely worked. The primary objective was expanding access and operational consistency quickly enough to support overwhelming demand.
In that environment, the systems that emerged were designed primarily around operational execution:
- Can providers schedule care?
- Can documentation be completed?
- Can claims be submitted?
Those were the right problems to solve at that moment. But the environment has now changed.
The economic visibility of autism care has increased dramatically. The aggregate spend is now large enough to attract materially greater scrutiny from payors and Medicaid programs.
Yet, the industry still lacks broad alignment around standardized efficacy measurement.
This isn't simply a technology problem. Autism is extraordinarily heterogeneous. The field still relies heavily on behavioral, operational, and administrative signals to infer treatment response indirectly. Session data and billing data alone were never going to solve the measurability problem.
This creates a structural tension.
If efficacy remains difficult to measure consistently while costs continue rising, the pressure to introduce other forms of utilization control increases — not because they are clinically ideal, but because they are operationally available.
One likely direction is a reimbursement environment where authorizations become increasingly dynamic rather than static. Instead of approving large blocks of care through periodic review cycles, payors may increasingly seek:
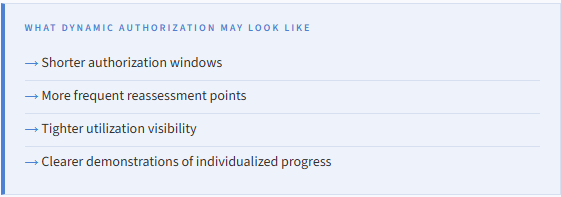
In this scenario, Prior Auth stops functioning as an administrative process and starts behaving like an ongoing operational intelligence function.
Providers will increasingly need infrastructure capable of connecting clinical documentation, treatment progression, authorization history, operational consistency, and reimbursement strategy into a coherent longitudinal view of care.
Not as disconnected administrative workflows. But as interconnected operational intelligence.
That may also place increasing pressure on platforms themselves. Systems historically optimized primarily around scheduling, documentation, and claims execution may face growing demand for tighter integration between care delivery, authorization management, longitudinal reporting, and payor-facing operational visibility.
Provider Readiness
Provider Impact
The pressure is obvious. The strategic responses are not.
But the next phase of autism care will likely involve far more emphasis on measurability, defensibility, and operational visibility than the industry has historically been required to support.
And that shift may arrive faster than many organizations expect.


